

All you need to know about 2019 coronavirus
- Mathias Talmant

- 4 avr. 2020
- 9 min de lecture
Dernière mise à jour : 4 avr. 2020
COVID-19 Series

In this article, I will try to answer the most basic questions that one may have about the current COVID-19 pandemic:
What is it?
Where does it come from?
How dangerous is it?
How to know if I am infected?
How to protect myself and my family?
When may the lowkdown come to an end?
Anatomy of the new coronavirus
First of all, let us call a spade a spade. As stated by the World Health Organisation, “SARS-CoV-2” is the name of the virus that causes the “COVID-19” disease (previously called 2019-nCoV). The coronavirus family was first identified in the 1960s and range from the common cold to more deadly diseases. There are more than 40 recognised crown-shaped viruses infecting a range of mammals and birds. However, spillovers can occur and allow diseases to follow across the species barrier into humans.
In 2002, the SARS-CoV (Severe Acute Respiratory Syndrome) jumped from a bat to a person by way of some intermediary and killed 800 people worldwide. Studies highlighted that the new coronavirus is very similar to the SARS-CoV, but COVID-19 is as different from the flu as we are from dinosaurs. On March 11, the new coronavirus took a global scale when it was updated from epidemic to pandemic by the WHO. The following video paints the portrait of the virus and its infectious mechanism.
Origins of the pandemic
SARS-CoV-2 emerged from Huanan, a live animal market in Wuhan, China in November 2019 – unsurprisingly, judging by the poor hygiene conditions of animal markets in China. In all likelihood, a turtle, a snake or maybe a pangolin was previously infected by a bat, which transmitted the disease to a human host and the rest is history. The analysis of public genome sequence found no evidence that the virus was human engineered.

Street vendor preparing a frog for sale in a Wuhan street market
Source: South China Morning Post
Strategically located on the Yangtze river and a few hours by train to most of China’s important cities, Wuhan (9,000,000 inhabitants) is a key transport hub for goods moving from China’s interior to coasts. This geographical situation coupled with mass migration over the Lunar New Year holidays and the fact that Chinese authorities took 23 days to alert WHO of a series of pneumonia-like cases in Wuhan laid the groundwork for a major outbreak. Nonetheless, it is worth noting a better reaction time from China, which took 86 days to notify WHO after SARS-CoV broke out in 2002.
Highly infectious but not so deadly
In the 14th century, the Black Death travelled from Asia to Crimea along the Silk Road. From there, infected fleas living on rats travelled on Genoese merchant ships, spreading throughout the Mediterranean Basin, reaching the rest of Europe via the Italian Peninsula. International trades and urbanisation facilitated the movement of germs among communities and across continents. Until here, the story sounds familiar and yet, doesn’t it? However, COVID-19 is very different from the Plague.

Dr Beaky of Rome, Paul Fürst (1721)
Notwithstanding the microbiological aspects, the lethality of the two diseases is simply not comparable. According to National Geographic, the plague killed an estimated 25 million people, almost a third of Europe’s population. The last three waves of Plague (VIth, XIVth, XIXth century) had a mortality rate ranging from 50% to 100% depending on the type of infection and whether if was treated or not. As a comparison, the fatality rate of Ebola, MERS-CoV and SARS-CoV were respectively 44%, 34% and 10%, but they only impacted a few thousands of cases. The new coronavirus is a lot more widely spread, but has a very light death toll compared to its peers. Call it Bird flu, H1N1, Ebola Global outbreaks are nothing new. All of these epidemics originated from animals and gained momentum as the end of the century XXI unfolded.
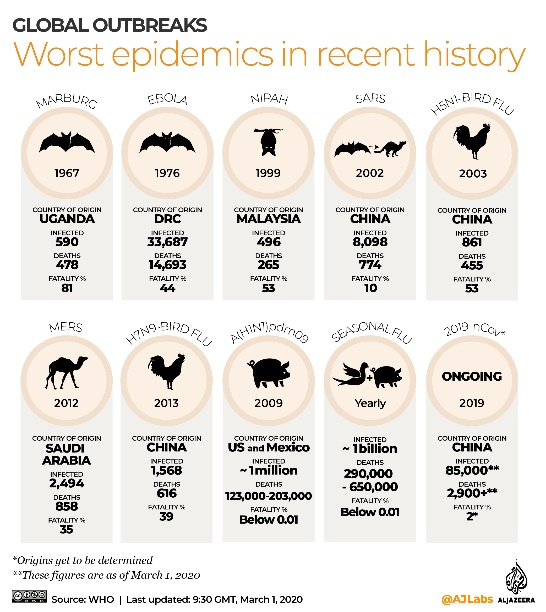
Today, “COVID-19” is on everyone’s lips because of its infectiousness and we are rightfully worried about the magnitude of this disease and how fast it has spread over the world. But as of early April, in relative terms, looking back at the worst epidemics in recent history, COVID-19 has a low case fatality rate (~5%). According to the WHO, the mortality rate of seasonal influenza is usually below 0.1%, which means that 290,000 to 650,000 people die of respiratory diseases associated with the flu globally each year. In other words, as of now, influenza’s death toll is still 5 to 12 times greater than COVID-19’s. It does not mean the ne coronavirus is not a threat, but figures must be put in perspective.

Source: South China Morning Post
Italy, Spain and France seem to be plateauing, but the UK and the US are still on a steep curve. China, which has one more month of data available, has successfully flattened the curve. India is only in the early stage and may the next major infection site. So far, South Korea proved to be the star pupil. This is partly explained by the country’s speed of reaction and massive testing campaign with “COVID-19 drive through”.

How a short-supply of swab is obstructing the world
The health fiasco we are experiencing in Europe more than anywhere else can be explained by our inability to deal with any of the three stages of the spread of the virus:
Before - A lack of authority in Western governments’ policies and mixed response from citizens, as opposed to more law-abiding Eastern citizens.
During – A lack of testing, which makes a notch in isolation efforts and foster the spread from asymptomatic carrier.
After - A lack of acute care hospital beds and ventilators to treat the disease.


Source: OECD, Financial Times (*US = 2016 data)
Currently there are two main reasons someone would be tested for the coronavirus: having symptoms or exposure to an infected person. France announced it would double its test capacity to reach 29,000 tests/day in early April, but is still far behind its German peer. Several health care giants such as Roche are doubling efforts to create fast COVID-19 testing machines to get a weight off medical laboratories, but as always, R&D and mass manufacturing take time. Besides, health care start ups are also try playing their cards. Hopefully, we will not end up with another Theranos-like machine. In the meantime, we can still rely on test kits.
The process is very simple and typically involves taking a swab from deep in a patient’s nasal cavity to collect cells from the back of the nose. The sample is then sent to a lab, where it will be tested to determine if the patient’s cells are infected with the virus. How does the test work? While collecting a sample is easy, interpreting the results is trickier. In order to detect the presence of RNA (the virus’ genetic material) in the patient’s sample, labs perform a test called reverse-transcription polymerase chain reaction. If genetic material from the virus is found in the sample, then the patient is infected. It takes 24-72 hours to get the results and although the test may not be 100% accurate, the benefits of testing outweigh the risk of an error.

Patient being tested for COVID-19
If we know how to diagnose COVID-19, why do European countries and the United States perform so little tests? The culprit is on the previous photo. It is not a mere cotton bud, but a highly specialised nasopharyngeal testing swab. The exploding need for them has created a bottleneck in the soaring demand for diagnoses and the two top makers, Copan Diagnostics (Italy) and Puritan Medical Products (USA), are located in some of the most impacted regions. Since the swabs are patented and specialized, they're hard to make on the fly. This adds to the list, among hydroalcoholic gel, masks, gloves and ventilators, for which governments are trying to ramp up production via a “war economy” against the virus. Initiatives to redirect manufacturing efforts are laudable, but they will take weeks to materialise and in the meantime the virus keeps spreading.
It is best to be tested in order to know if you are a silent spreader, but given the short supply of test kits, especially in Europe, you should only be tested if you feel sick or if you have been in contact with an infected individual. With a view to reducing congestion in hospitals, practice SELF-DIAGNOSIS BUT NO SELF-MEDICATION. Media are talking a lot about possible cure such as Chloroquine, but there may be side effects and authorities have not approved any treatment yet. Stay home and if you feel the symptoms presented hereafter, use telemedicine or go to the hospital.

Source: South China Morning Post
Hands off and put down the masks




Source: South China Morning Post
Masks are in such short supply worldwide and retailers increased their price tag by up to twenty-fold. Hongkongers have been queing overnight for more than 10 hours to buy them. Governments are severely blamed for not having anticipated the massive need for surgical masks on the eve of the outbreak, but this is not the main setback. While masks such as the N95 respirator offer some protection, coronavirus particles are small enough to pass through most surgical mask filters.
It is reassuring for many citizens to wear surgical masks, but let us not forget that they are initially designed to prevent surgeons from infecting patients’ wounds and not the other way around. Surgical masks provide little protection against COVID-19, but it is safe to say that they are good for one thing: preventing you from touching your nose and mouth with your fingers.
Assuming that the virus can only spread via respiratory droplets and infected surfaces, N95 respirators (rigid face masks) might play a bigger role, because they can filter particles up to 0.3 microns in diameter. However, a recent study published in the New England Journal of Medecine did not exclude the risk of aerosol transmission. This refers to extremely small airborne particles that travel longer distances and can stay suspended in the air for hours. With aerosols masks would be useless and even the six-foot distance would be questionable, but scientists have not agreed yet.
In conclusion, wearing a mask provides no guarantee to be spared by the virus, yet it has some benefits. Given the short supply, all masks should be supplied first to medical staff and sick people. For the rest of us, it is possible to make our own mask as showed in this video. According to Hong Kong’s Consumer Council, homemade masks achieved 90% of the filtering functions of surgical masks. The best ways to be safe is to stay at home and frequently clean your hands with alcohol-based hand rub or washing or soap and water. No reported cases of COVID-19 have been linked to food contamination yet. To avoid fake news, please refer to WHO website for reliable and up to date information.
Way more than a 40-day quarantine
As sad as it may sound, this summer you are more likely to do “home farniente” than beach sunbathing. As mentioned in my previous article where I modelled several scenarios for the COVID-19 outbreak, the infection peak could be reached on July 15, 2020 and less than 1% of the world population would be spared by COVID-19, leading to a total cumulative number of deaths of 231,266,604 deaths in late March 2020. Herd immunity would be reached by vaccinating 86% of the world population. This is near impossible to reach, especially over a year. This involves many assumptions, but day after day it seems more realistic.

Source: Financial Times
As evidenced, by this timeline from the FT, the spread virus is showing no slowing down in Europe. Obviously, this situation will eventually come to an end after we reach the peak, but when? Data reported by China point toward a recovery two months after the inflection point. Knowing that Chinese premier Li Keqiang had to warn local governments not to cover up new cases of Covid-19, I am not personally convinced of China’s data veracity. I am currently looking for a job and several companies I have been talking with in Europe have frozen their hiring process until September.
Globally, if we see a peak in June/July, I do not expect quarantines to end before August or September. This implies at least four more months of global shutdown. As Bill Gates said: “If we do it right, we'll only have to do it once” and this brings me to my very last point. After reporting no new domestic cases in mid-March, China dropped its guard and immediately experienced a resurgence from new imported cases. The global economic, social and educational impact will be very bad, but me must grit our teeth if we want to avoid a second wave. We can be sure, and this is understandable, that as soon as governments declare the end of the lockdown, everyone will rush off to go to bars, cinemas and restaurants. Therefore, governments must make sure that the inflection point is way past and that they have enough acute care hospital beds, testing kits and other health supplies before they open up the economy. This will take months, but it is the price to pay for safety and stability.
The above references an opinion and is for information purposes only. It is not intended to be investment advice. Seek a duly licensed professional for investment advice.
MT Finance - Mathias Talmant.



Commentaires